Resources
Most of what we do is not available publicly, but we’re proud of what we can share
Most of what we do is not available publicly, but we’re proud of what we can share
This issue brief builds off the Rare Access Action Project’s (RAAP’s) 2025 paper, “Solving for Access and Affordability: PDABs are Not the Answer” and explains why borrowing the Maximum Fair Price benchmark price for state prescription drug affordability boards (PDABs) would recreate the same legal, operational, and access problems already observed with any use of upper payment limits (UPLs). When removed from Medicare’s statutory framework, MFP functions as a reimbursement ceiling (the same as any UPL), with consequences that show up in patient access and care delivery.
States are under increasing pressure to respond to concerns about prescription drug affordability. In that search for solutions, Medicare’s MFP has begun to surface as an attractive model for state efforts. MFP is highly visible and branded as “negotiation,” giving it the appearance of a tested and defensible pricing tool.
That appeal is understandable. But it is also misleading.
Medicare’s MFP does not function as a standalone benchmark. It works only because it is embedded in a federal program with national scope, statutory carve-outs, and the ability to redesign coverage and payment rules around the negotiated price. Those features are not transferable to state markets and MFP has the same problems as any other UPL benchmark.
This issue brief was commissioned by the Rare Access Action Project.
While the nation’s health spending is high, it is tempting to blame the cost of prescription drugs. After all, prescription drugs are one of the most visible costs to patients. However, only 13% of costs can be attributed to prescription drugs and much of the utilization is in generic drugs which are less expensive in the U.S. than in other countries. Overall, prescription drugs provide immense value that extends far beyond their direct cost, acting as a high-return investment in national health and economic vitality.
Prescription drugs not only manage chronic diseases and improve quality of life for millions but also drive significant cost savings by preventing more expensive hospitalizations and emergency room visits. Furthermore, by improving patient health, these treatments boost productivity, contribute billions to the economy, and extend lives.
To improve affordability and access, policymakers need to work toward policies that balance pharmaceutical innovation with equitable access, ensuring that the U.S. continues to reap the long-term societal benefits of these vital medical advancements.
This issue brief was commissioned by the Alliance for Patient Access (AfPA).

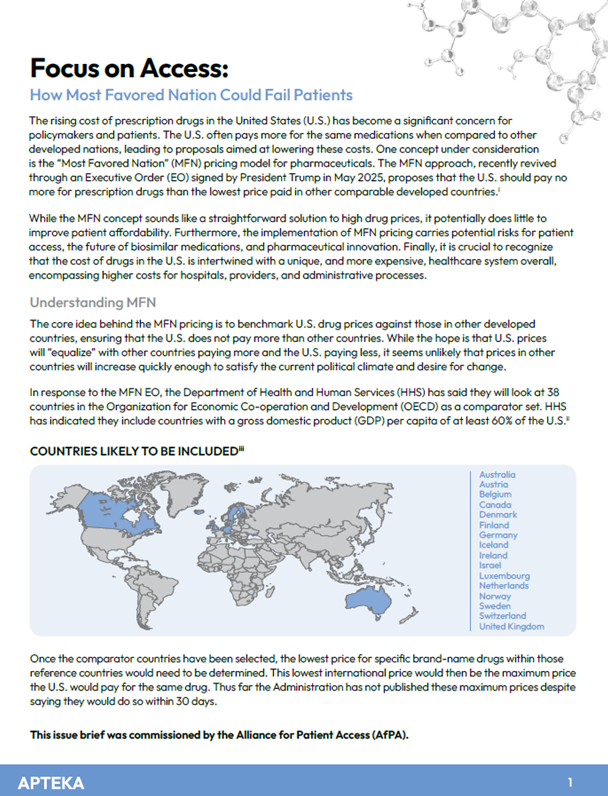
While the concept of Most Favored Nation sounds straightforward, it potentially does little to help patient affordability. Furthermore, it could carry risks for pharmaceutical innovation and U.S.-based research and development.
A deeper look at the concept of MFN reveals its significant limitations in addressing the core issue of patient affordability and access. Prescription drugs in the U.S. are aligned with the value they provide in relation to other healthcare costs, and we are right in line with other countries: 9% of United Kingdom’s National Health Service budget goes to medicine compared to 17% in Germany and Italy and 15% in France.
To truly address patient affordability, policymakers need to consider more comprehensive reforms that tackle all aspects of healthcare costs including enhancing transparency in the drug pricing and insurance system and ensuring that any savings achieved are directly passed on to patients at the point of sale. A singular focus on MFN pricing risks undermining pharmaceutical innovation and market dynamics without guaranteeing meaningful relief for American patients struggling to afford their medications.
This issue brief was commissioned by the Alliance for Patient Access (AfPA).
Theory has not matched reality and the implementation of PDABs has revealed difficulties in achieving its lofty goals and has led to concerns about unintended consequences. A quick legislative win creating a PDAB can, overall, mean little to the state or its residents because the healthcare system is incredibly complex, and savings may prove illusive.
PDABs are not necessarily equipped to foresee the unintended consequences of their actions, particularly for patients with rare diseases, providers, hospitals, health centers and community pharmacies. Nowhere is this more apparent than with the PDABs that are moving towards implementation of Upper Payment Limits (UPLs). While the return on investment for PDABs is questionable overall, the challenges of implementation are considerable and the pay-off for patients is limited at best – particularly as we consider the use of UPLs.
Apteka worked with RAAP (the Rare Access Action Project) to dive into the world of PDABs and UPLs to illustrate why they haven’t gone the way legislators hoped and why they are a threat to patients, particularly those with rare disease.
Link to Executive Summary (Focused on PDABs and Rare Disease)
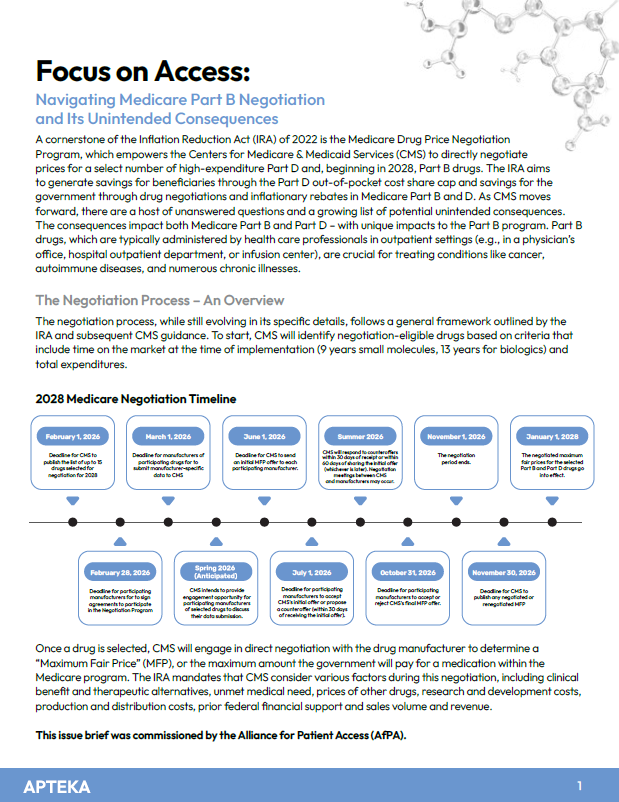
The Medicare Drug Price Negotiation Program empowers the Centers for Medicare & Medicaid Services (CMS) to directly negotiate prices for a select number of high-expenditure Part D and, beginning in 2028, Part B drugs.
As CMS moves forward, there are a host of unanswered questions and a growing list of potential unintended consequences. The consequences impact both Medicare Part B and Part D – with unique impacts to the Part B program.
The path to operationalizing Part B negotiations is fraught with complexities. The mechanics of determining the Maximum Fair Price, the challenge of implementing new reimbursement models, and the potential for unintended consequences – particularly the impact on Average Sales Price and provider viability – demand careful observation and adaptation. Maybe most importantly, the impacts on beneficiaries will become clearer but limited access, increased direct costs, changes in site of care and access to new therapies are all legitimate concerns.
This issue brief was commissioned by the Alliance for Patient Access (AfPA).

Is the biosimilars market working? Apteka was commissioned by Alliance for Patient Access and the Biologics Prescribers Collaborative to examine if, almost a decade since the first approved biosimilar in the U.S., are biosimilars are achieving three objectives: (1) decreasing costs to the overall health care system, (2) increasing patient access/options, and (3) reducing patient cost sharing.
Beyond those objectives, what are the barriers to realizing the full potential of biosimilars? What policies have helped or hindered the market, and are some payers doing better than others? And, given the findings, what are the recommendations that would lead to a more stable and robust biosimilar market?
The IRA enacted the most significant changes to Part D since its inception, and these reforms have major implications for Medicare beneficiaries. In this new paper, the MAPRx Coalition examines the potential impact of three of IRA’s major Part D provisions.